Arleen Cozart
Arleen Cozart
Blog
About
Contact
Blog
About
Contact
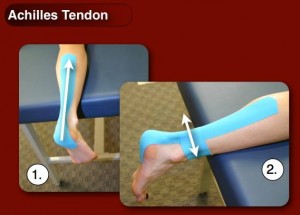
 Pain of the Achilles tendon commonly affects both competitive and recreational athletes, and the sedentary. The largest tendon in the body, the Achilles tendon, endures strain and risks rupture from running, jumping, and sudden acceleration or deceleration. Overuse, vascular diseases, neuropathy, and rheumatologic diseases may cause tendon degeneration. The hallmarks of Achilles tendon problems seem to be damaged, weak, inelastic tissue.
Pain of the Achilles tendon commonly affects both competitive and recreational athletes, and the sedentary. The largest tendon in the body, the Achilles tendon, endures strain and risks rupture from running, jumping, and sudden acceleration or deceleration. Overuse, vascular diseases, neuropathy, and rheumatologic diseases may cause tendon degeneration. The hallmarks of Achilles tendon problems seem to be damaged, weak, inelastic tissue.